
The Biopsychosocial Model of Pain: Why Your Body, Brain, and Stress Levels All Decide How Much You Hurt
Pain is such a complex topic.
It can also be pretty complex to treat. Over the years as a sports chiropractor, I’ve realized my role extends much farther than just treating musculoskeletal pain.
Don’t worry - I stay within my scope. I know when to refer out, and when I can treat. So do keep that in mind as you read on.
When I say my role extends much further… I’ve realized I have to give people confidence that they can get out of pain more than anything else. It sounds kind of silly, but the mind is a powerful tool. Arguably more powerful than any actual structural damage.
I give this example all of the time: “If someone were to come work with me thinking they will never get out of pain, then they are right.”
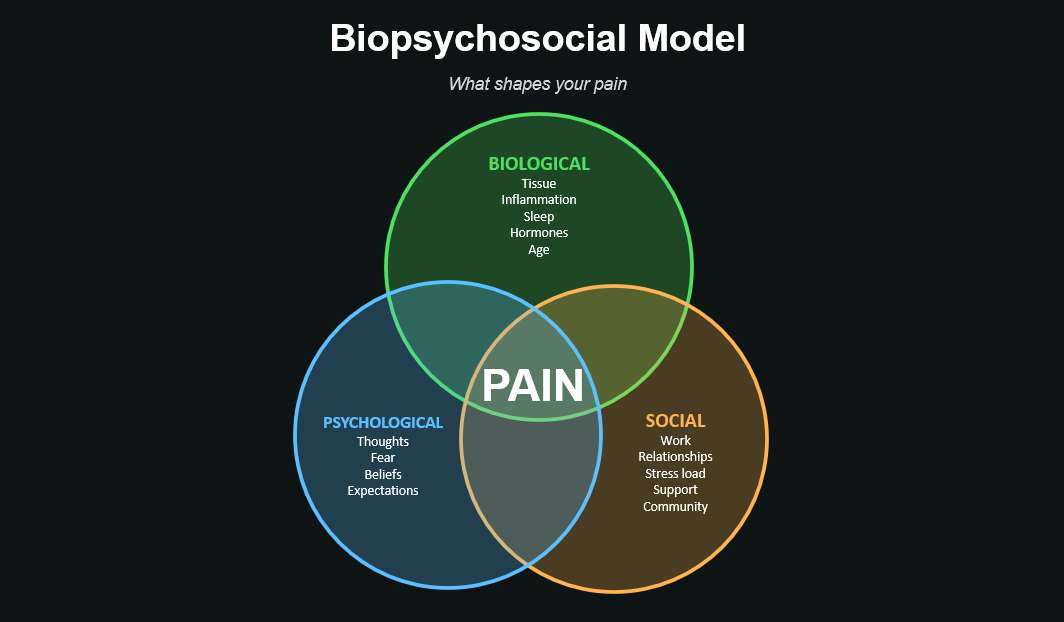
So… what’s this model I’m talking about? The Biopsychosocial Theory was first proposed in the late 70s, but not until the early 2000’s did it get developed into a clinical tool. The idea is that any health condition, including pain, is shaped by three overlapping domains:
Biological: the tissue itself, inflammation, nerve signaling, hormones, sleep, age
Psychological: thoughts, beliefs, fears, expectations, mood, attention, stress
Social: work environment, relationships, financial stress, support system, culture
When I have a new client, I’m plotting where their pain falls on this model in my brain. I’m assessing the structure/tissue (Biological) through a physical exam, the Psychological & Social components through their health-history and by talking with them. I’m asking them questions like: “how bad does it hurt?”, “do you think you’ll ever feel better?”, “what do you do for fun?”, “How is this impacting that?” Those things help me get a good gauge of where they plot on the Venn-Diagram.
Here are a few good examples:
Example 1: Let’s say a client’s pain is structural. Tissue is inflamed, and it needs to calm down. But the client is absolutely freaking out about it. Well, that will only make things worse. I can educate them on how this is going to go away in a few days or weeks, and give them tools and tips on how to go about that. Aka, address the psychological component of their pain.
And boom! They get better.
OR
I can feed into it. “Yeah, this is bad. You’ll always have this issue as long as you live.”
And boom! I become rich in the worst way possible, because I told you your pain was never going to go away.
Example 2: You know when you hear those awesome success stories where someone says: “The doctor said I’d never work out again without pain, but I did it.”
Well it’s truly amazing. But if we want to really break that down, what if the doctor misdiagnosed their pain to begin with? They thought it was a structural issue that couldn’t be resolved, so they said that.
Turns out, it was never structural. But the doctor’s comments actually made it psychological. So really, their pain got better with time (as most pain does), and they overcame the psychological barrier of a medical professional telling them they’d never work out again without pain.
And if the doctor would have just told them that to begin with, then they would never have had to go through the emotional turmoil of dealing with their pain.
But then again, what if this was a great lesson that they needed to learn, that they could overcome hard things…
(Talk about a mind twister).
Example 3: The doctor tells you to rest because of an injury.
I’ll put this one on the record: That’s a cop-out, 99% of the time.
Pain isn't a bad thing… (you should check out the last blog I did). But now that the doc told you to rest, you aren’t going to your fitness class anymore. And that’s where your friends are. That’s how you relieve stress. That’s how you clear your mind.
But not anymore. Now, you’re coming home earlier. Maybe stopping by a fast-food restaurant on your way home. Maybe drinking those extra few beers now when you could’ve been working out.
Now, the “Social” component of your pain is being impacted.
What if we worked on ways on keeping you in your fitness class instead? Educating you on how to modify? Educating you on how to approach pain when you have it in your class/activity?
Example 4: Easiest one yet. You know when a toddler takes a nasty fall and looks at you like they are about to cry? And how you’re supposed to tell them they are tough and that they can shake it off and be fine?
And if you do that, they are fine? But if you give into it, then they cry?
Well, we are the same way. We are toddlers…
This isn't a psychology lecture. This is anatomy. Stress and emotional state physically change how the spinal cord processes pain. Your brain has a built-in dimmer switch on incoming pain, and life conditions decide which way it's turned.
A few practical translations.
1. Imaging doesn't tell you why you hurt. A bulge on a scan is one data point, not the whole story. (More on this in the next post.) A disc bulge in someone who's slept well, lifted consistently, and feels in control of their work doesn't behave the same way as the same bulge in someone who hasn't.
2. The fix isn't always tissue work. Sometimes the most useful thing for chronic pain isn't another set of stretches. It's sleep. Or fewer overtime hours. Or finally getting help with the anxiety that's been building for two years. I've watched chronic low back pain disappear in people who didn't change a single exercise. They changed something else.
3. Move anyway. One of the most powerful interventions in pain science is graded exposure. Slowly loading the area that hurts, in safe ranges, while the nervous system learns it's not in danger. Rest doesn't usually help chronic pain. Controlled movement does. (Acute pain is a different story. If something is freshly broken or torn, the answer is different.)
4. Your story matters. If you've been told "your back is degenerated" or "your disc is bulging," your brain takes that information and uses it to predict future pain. Words shape outcomes. The same finding described as "normal age-related changes" produces less pain and faster recovery than the same finding described as "degeneration."
The biopsychosocial model isn't telling you the pain is in your head. It's telling you that pain is real AND that it's shaped by more than just tissue. Both things are true at the same time.
The people who make the biggest jumps in my office aren't training more - they're sleeping an extra hour, dropping the catastrophic thinking, and treating pain as data.
Once you accept that pain isn't always damage, the question becomes "what IS it then?" And the answer is almost always some combination of biology, psychology, and the life you're currently living.
Treat all three.
If you enjoy these posts - share with a friend! I write these purely to help educate - we’d love for you to explore around on our website for all of our offerings!
Thanks,
Dr. Lee Pinkham, D.C., CF-L2, A.R.T.