
The Truth About Your MRI: When the Image Doesn’t Match the Pain
What is your MRI really telling you about your pain?
Usually a lot less than you think...
How often have you heard this? (Or maybe even said it)
“Yeah, the doctor said the MRI said I have a disc (degeneration/bulge/protrusion and have a bad back so I can’t do any (insert anything physically demanding).”
What if… that finding on the MRI was already there?
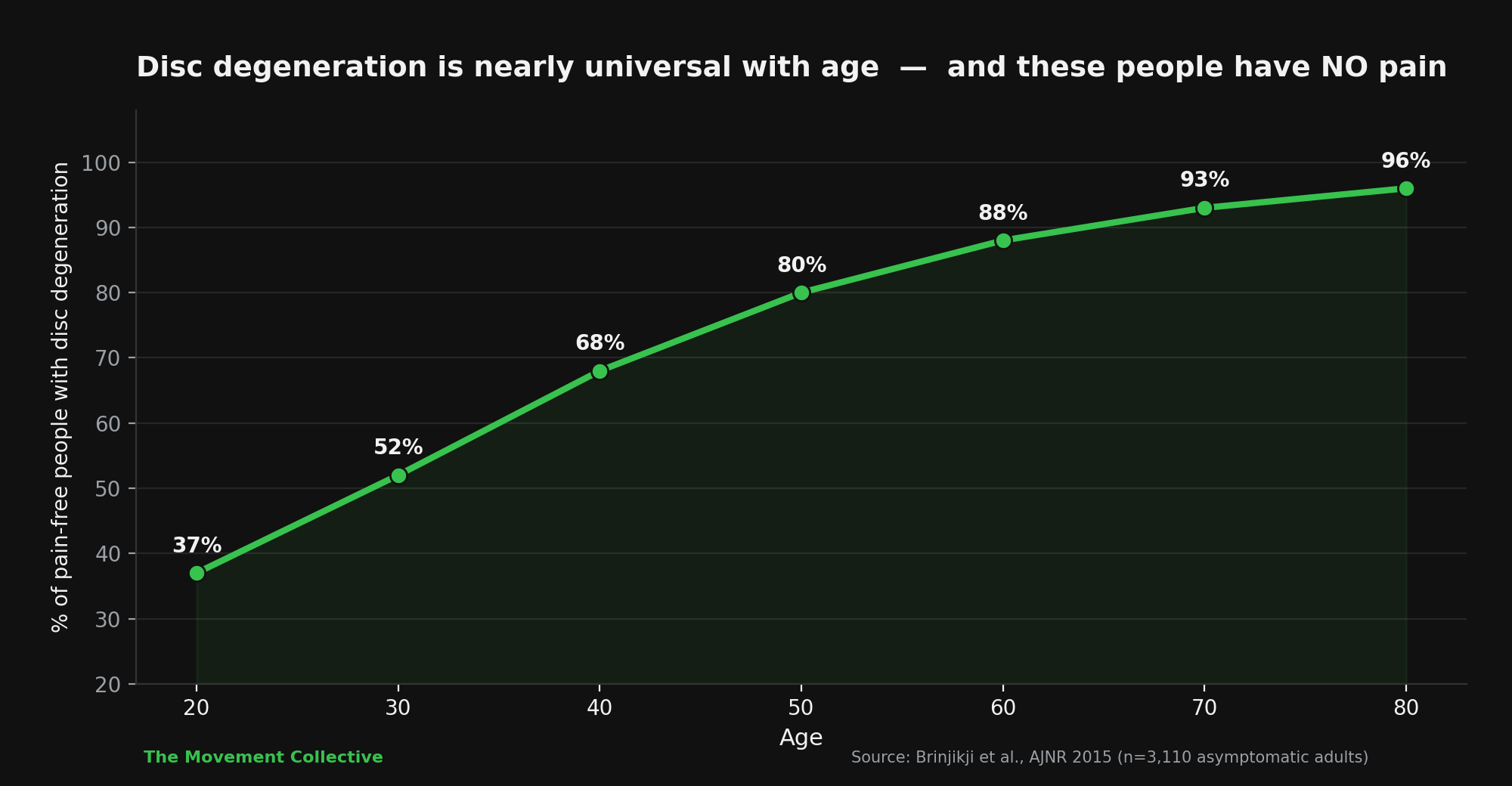
In a study of more than 3,000 people who had zero pain, 37% of the 20-year-olds had disc degeneration on their MRI. By age 50 it was 80%. By age 80 it was 96%. The same imaging finding that everyone gets told causes their pain. Found in nearly every healthy older adult in the room.
The picture on the screen and the pain in your body are not the same thing. And misunderstanding that gap is one of the biggest reasons people never get better.
In 2015, Dr. Waleed Brinjikj at the Mayo Clinic ran a systematic review pulling together 33 separate studies on people who had no back pain and had gotten an MRI. The total sample was 3,110 asymptomatic adults. What they found was pretty substantial.
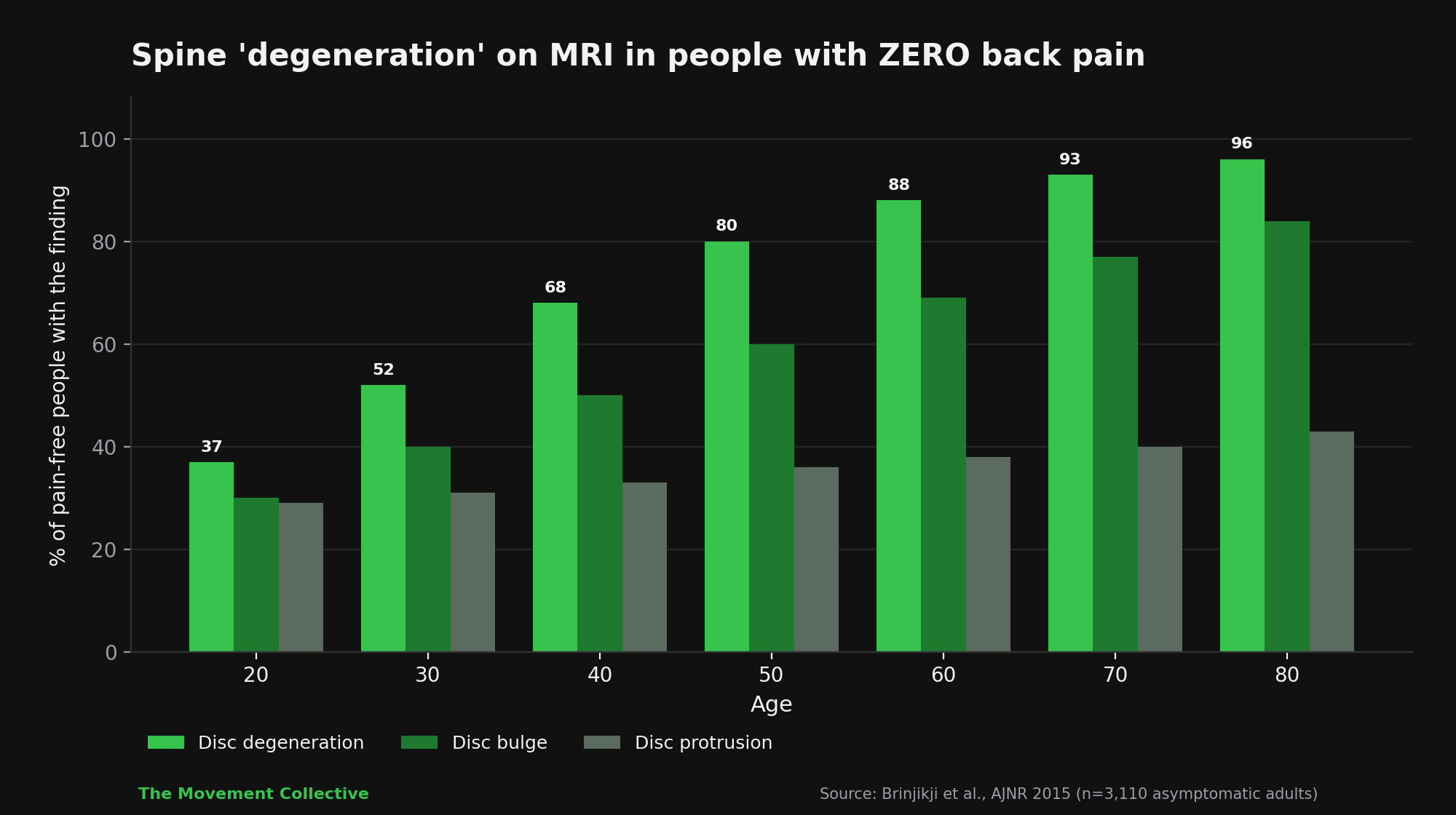
Here’s the breakdown by age in people with zero back pain:
Age 20: disc degeneration 37%, disc bulge 30%, disc protrusion 29%, annular fissure 19%
Age 30: disc degeneration 52%, disc bulge 40%, disc protrusion 31%, annular fissure 20%
Age 40: disc degeneration 68%, disc bulge 50%, disc protrusion 33%, annular fissure 22%
Age 50: disc degeneration 80%, disc bulge 60%, disc protrusion 36%, annular fissure 23%
Age 60: disc degeneration 88%, disc bulge 69%, disc protrusion 38%, annular fissure 25%
Age 70: disc degeneration 93%, disc bulge 77%, disc protrusion 40%, annular fissure 27%
Age 80: disc degeneration 96%, disc bulge 84%, disc protrusion 43%, annular fissure 29%
Remember - these are people without pain. The findings most of us have been told are “causing” our pain are present in basically every healthy person over 50.
Please understand that this doesn’t mean a MRI is useless. MRI is a critical tool. If you have red-flag symptoms (loss of bowel or bladder control, progressive neurological deficits, suspected fracture, suspected infection or tumor), an MRI is essential. Get the imaging.
This also doesn’t mean disc bulges never cause pain. They can. A separate analysis the same year showed that disc extrusions, spondylolysis, and certain Modic changes WERE more common in people with low back pain than without. Some imaging findings do correlate with pain. Most don’t.
What this means is that imaging alone cannot tell you whether your specific finding is the cause of your specific pain.
Here’s how it typically plays out in the office.
A patient comes in with low back pain. They’ve had an MRI. The report says “L4-L5 disc bulge with mild facet hypertrophy.” They’ve already been told by someone, somewhere, that this is the problem. They’ve been moving carefully, avoiding loading, sleeping in a special way, doing some stretches they found on YouTube. Maybe even an injection of sorts to help with the pain as well.
And aren’t getting better.
I see the images, but I’m looking at them. I’m asking different questions. Where does it hurt? When did it start? What movements provoke it? What relieves it? Does it radiate? What does it feel like at the end of a long day vs. first thing in the morning? Are you sleeping? What’s your stress like? How much load can you tolerate before symptoms increase?
About 70% of the time, the imaging finding is incidental. Their back hurts because of something else entirely. A movement pattern they’ve been protecting for months. A loss of hip extension. A stress-loaded nervous system. A loss of the kind of varied movement most adult bodies need to stay happy. The disc bulge is sitting there, exactly like the disc bulge in 60% of pain-free 60-year-olds.
When we treat the movement pattern, sleep, and the loading capacity, the pain resolves.
The disc bulge is still on the MRI. They just don’t notice it anymore.
Three things to take away:
1) An MRI is a snapshot of structure, not function.
It shows you what tissue looks like. It cannot show you whether that tissue is generating your pain. Your symptoms, movement testing, and history do that.
2)Nocebo is real.
When you’re told you have a “degenerated disc,” your brain takes that information and uses it. Studies show that patients given more dramatic interpretations of imaging findings have worse outcomes, higher pain ratings, and longer recovery times than patients given the same findings described in neutral language. Words shape outcomes.
3) Get a second opinion if the recommendation is invasive.
If someone is recommending surgery, injections, or major intervention based primarily on imaging findings, get a second opinion. Especially if those findings include words like “degenerative” or “bulging.” Those words describe normal aging in most people over 40. They may or may not have anything to do with your symptoms.
What an MRI is good for
To be clear, I order imaging and/or refer out when it changes the plan. Specifically: suspected fracture, infection, etc. Progressive neurological deficits (worsening weakness, numbness, reflex changes). Failure to improve with appropriate conservative care after 6 to 12 weeks. Surgical planning, when surgery is on the table.
If none of those apply, the MRI usually doesn’t change what I recommend. The treatment plan is built off the exam, movement testing, and history. The imaging confirms or rules out things. It doesn’t usually drive the plan.
So one more thing…
The next time someone tells you your MRI “looks bad,” ask two follow-up questions. First, “what specifically is the finding?” Second, “what percentage of asymptomatic people my age have this same finding?” Most providers don’t know that second answer. Now you do.
Imaging is a tool. Use it. Don’t let it use you.
Want to go deeper? Read Pain is data, not always damage and The Biopsychosocial Model of Pain. And if you’re not sure where your own body stands, take one of our free self-assessments.
References
Brinjikji W, Luetmer PH, Comstock B, et al. Systematic literature review of imaging features of spinal degeneration in asymptomatic populations. American Journal of Neuroradiology. 2015;36(4):811-816. https://www.ajnr.org/content/36/4/811
Brinjikji W, Diehn FE, Jarvik JG, et al. MRI findings of disc degeneration are more prevalent in adults with low back pain than in asymptomatic controls: A systematic review and meta-analysis. American Journal of Neuroradiology. 2015;36(12):2394-2399. https://www.ajnr.org/content/36/12/2394
Boos N, Rieder R, Schade V, Spratt KF, Semmer N, Aebi M. The diagnostic accuracy of magnetic resonance imaging, work perception, and psychosocial factors in identifying symptomatic disc herniations. Spine. 1995;20(24):2613-2625.
Darlow B, Dean S, Perry M, et al. Easy to harm, hard to heal: patient views about the back. Spine. 2015;40(11):842-850.